Testing and treatment of uterine fibroids (1) Surgery and medications
Healthcare
About This Information:
This English version is a translation of content originally created based on medical information used in Japan. Accordingly, the data and treatment approaches presented reflect the situation in Japan and may differ from those in other countries or regions.
Supervised by: Dr. Megumi Yokota (Lecturer, Department of Obstetrics and Gynecology, Hirosaki University Graduate School of Medicine)
Testing and diagnosis of fibroids
Uterine fibroids are often discovered during a gynecological examination or on imaging tests. They are sometimes discovered for the first time during prenatal checkups. After reviewing the patient's symptoms and the condition of the uterus, the following tests are performed as needed.
Pelvic examination
The doctor manually examines the size, shape, and firmness of the uterus. If fibroids are present, the uterus may feel enlarged or firmer than usual.
Ultrasonography (ultrasound)
Using a probe (a device that produces images of the inside of the body by applying ultrasound waves), the doctor examines the uterus either through the abdominal wall or with a thin probe inserted into the vagina. Ultrasound allows for detailed assessment of the size, number, and location of fibroids.
Hysteroscopy (uterine fiberscopy)
In hysteroscopy, a thin camera (the hysteroscope) is inserted into the uterus through the vagina to allow direct examination of the uterine cavity. It is particularly useful when a submucosal fibroid protruding into the uterine cavity is suspected.
MRI
When ultrasound alone is not sufficient for diagnosis, MRI is performed to examine the location and characteristics of fibroids in more detail. It is often used when surgery is being considered.
Blood test
For women with heavy menstrual bleeding, a blood test is performed to check for anemia. Tumor markers may also be measured to help rule out malignancy.
Fibroid treatments
Several options are available to treat fibroids.
The choice of treatment varies from woman to woman, depending on the severity of symptoms, age, whether she hopes to become pregnant in the future, and whether she wishes to preserve the uterus. Because fibroids are benign, mild cases can often be managed with monitoring alone, without active treatment. However, treatment may be considered when fibroids interfere with daily life or cause severe anemia.
Treatment of fibroids falls broadly into two categories.
(1) Surgical treatment
This approach involves removing either the fibroids themselves or the entire uterus. By directly removing the source of symptoms, surgery reduces the risk of recurrence and offers strong therapeutic results.
(2) Non-surgical treatment and medication
These approaches include medications that control symptoms by regulating hormonal balance, as well as procedures that shrink or destroy fibroids without requiring abdominal incisions.
When deciding which approach is right for you, it is important to discuss the options with your doctor and choose one that fits both your physical condition and your personal preferences.
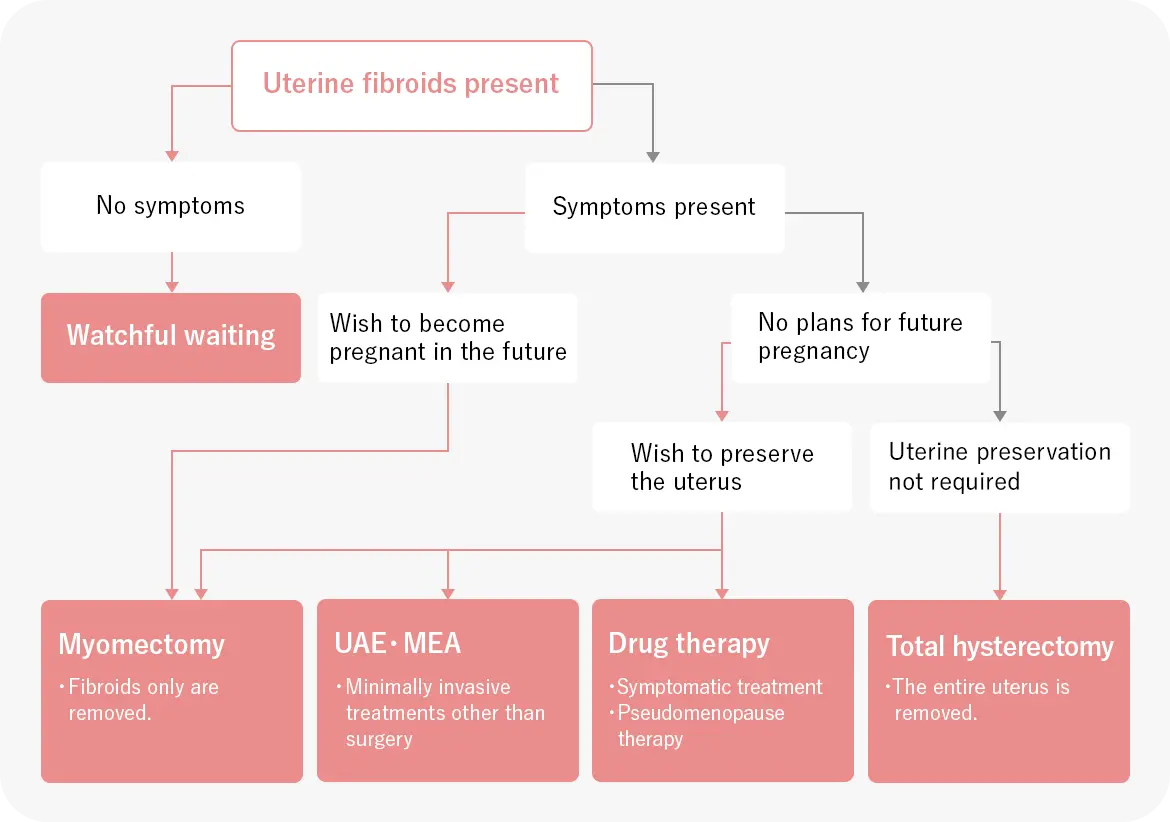
How to think about choosing a treatment
Myomectomy
In a myomectomy, only the fibroids are removed, while the uterus itself is preserved. It is often chosen by women who hope to become pregnant or who wish to keep their uterus.
-
Features
Because the uterus is preserved, myomectomy is the first choice for women who hope to become pregnant and give birth in the future. It is also a suitable option for women who wish to keep their uterus regardless of whether they plan to become pregnant. -
Points to consider
Any small fibroids that were too small to detect at the time of surgery may grow and cause a recurrence several years later. Because the uterus is sutured during surgery, subsequent deliveries are generally recommended to be by cesarean section. -
Main surgical methods
Laparotomy, laparoscopic surgery, and vaginal surgery -
Typical length of hospital stay
Usually about 3 days to 1 week. -
Suitable cases
Women who wish to become pregnant; cases where fibroids are large
The surgical method varies depending on the size and location of the fibroids.
|
Laparotomy (open abdominal surgery) |
Performed when fibroids are large or numerous. |
|---|---|
|
Laparoscopic surgery (performed through small abdominal incisions) |
Performed through several small incisions in the abdomen. Recovery is quick and scarring is minimal. |
|
Hysteroscopic surgery |
Performed for fibroids located inside the uterus. Because instruments are inserted through the vagina, no abdominal scarring occurs. |
Total hysterectomy
A total hysterectomy removes the entire uterus, eliminating the underlying cause of the condition. It is performed when fibroids are large, or when symptoms are severe and other treatments are not viable.
-
Features
This treatment eliminates any concern about recurrence and resolves symptoms such as heavy menstrual bleeding, menstrual pain, and anemia. It also removes the future risk of uterine cancer (both endometrial and cervical), which can provide additional peace of mind. -
Points to consider
Because the uterus is removed, future pregnancy and childbirth are no longer possible. If the ovaries are left in place, female hormone production continues, so menopausal symptoms do not appear immediately after surgery. -
Main surgical methods
Options include laparotomy (open abdominal surgery), laparoscopic surgery (surgery through small incisions), and vaginal surgery. In recent years, robot-assisted minimally invasive surgery, which places less strain on the body, has also become available. -
Typical length of hospital stay
Usually about 1 to 2 weeks. -
Suitable cases
Severe symptoms; cases where other treatments are not viable; women with no plans for future pregnancy; women who wish to eliminate any concern about recurrence
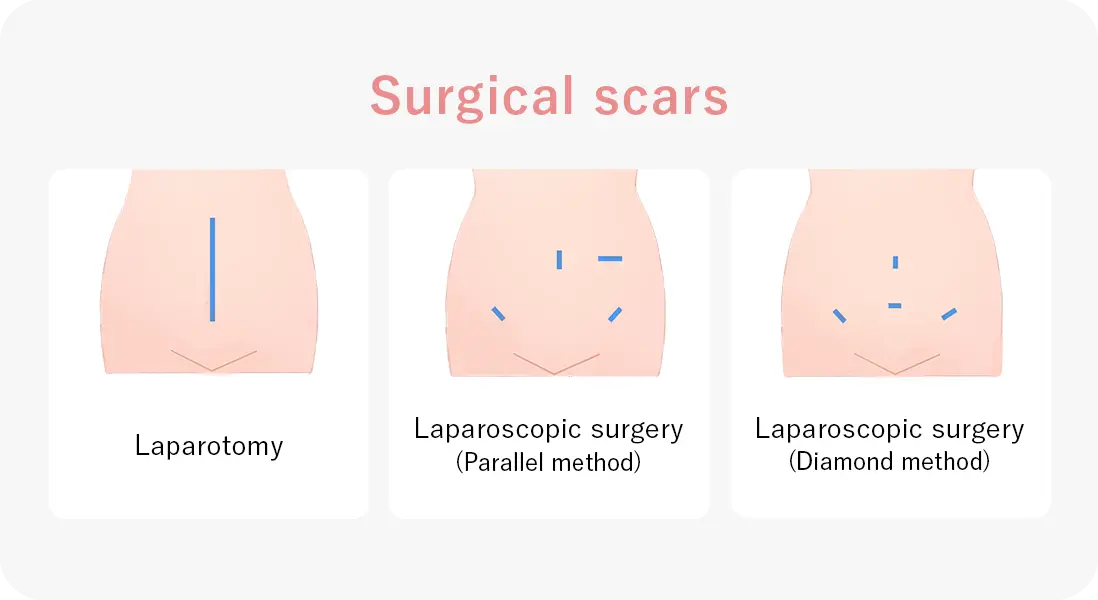
Surgery performed without making large abdominal incisions
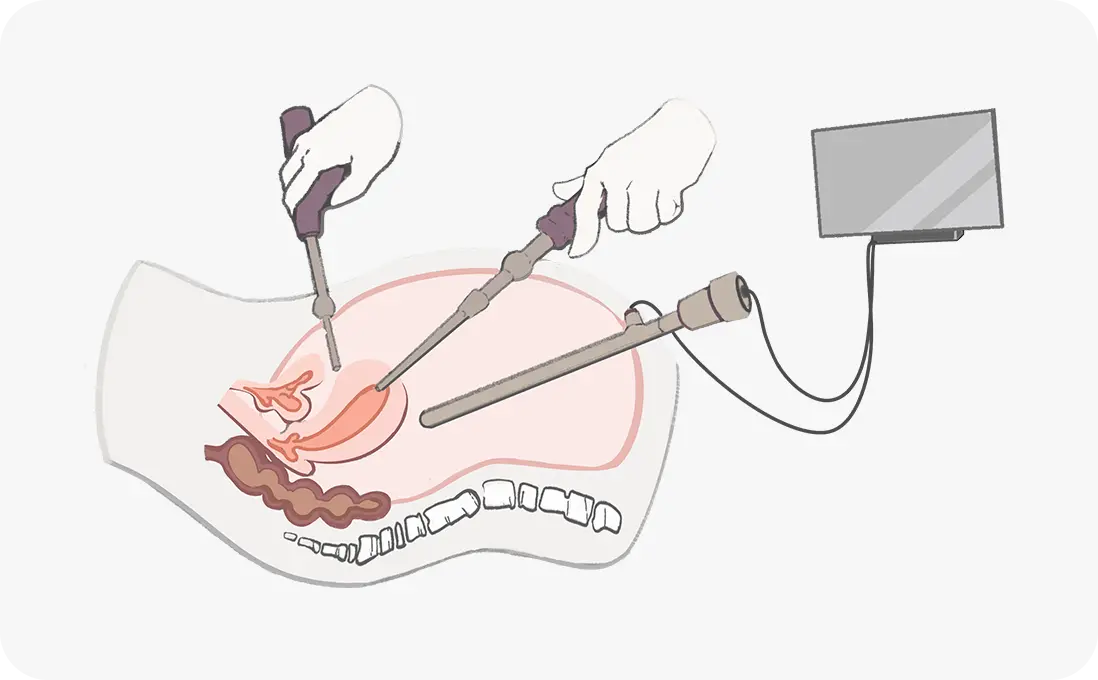
Laparoscopic surgery
In laparoscopic surgery, several small incisions, about 5 to 10 mm long, are made in the abdomen, and a camera (the laparoscope) and thin instruments are inserted through them. The abdominal cavity is slightly inflated with medical-grade carbon dioxide gas, and the surgeon operates while viewing images of the interior on a monitor.
Because no large incisions are made, laparoscopic surgery involves less bleeding, milder pain, and faster recovery. Patients are usually able to leave the hospital within a few days and return to their daily lives soon afterward.
In gynecology, laparoscopic surgery is used not only for uterine fibroids but also for conditions such as endometriosis, ovarian cysts, and ectopic pregnancy. It is also widely used for digestive conditions such as gallstones and appendicitis, and for urological conditions involving the kidneys and adrenal glands. Today, it is widely recognized across many medical fields as one of the gentler approaches to surgery.
Drug therapy
Two types of drug therapy are available: symptomatic treatment to relieve symptoms, and pseudomenopause therapy, which suppresses female hormones to temporarily shrink fibroids.
-
Symptomatic treatment
Symptomatic treatment aims to relieve distressing symptoms such as menstrual pain and bleeding. Treatment may include pain relievers, iron supplements or other medications for anemia, and hormonal agents that reduce bleeding by regulating hormonal activity. These are often used in combination. While these medications do not reduce the size of the fibroids themselves, they can be effective for mild symptoms. -
Pseudomenopause therapy
Pseudomenopause therapy uses medication to temporarily suppress the secretion of female hormones, creating a state similar to menopause in order to shrink the fibroids. It may also be used as a pretreatment to shrink fibroids before surgery. Because long-term use increases the risk of osteoporosis, this therapy is generally limited to a maximum of six months. -
No hospital stay
Outpatient treatment -
Suitable cases
Mild symptoms; women who wish to bring their symptoms under control temporarily